

Some people remain clueless about female genital anatomy and for good reason, as they’ve likely had no formal instruction on the topic. Education often involves knowledge imparted from friends and schoolmates and perhaps a talk from a parent on the “birds and the bees,” generally less than adequate means. “Sex Ed” classes in junior high school (a.k.a. middle school) were cursory and insufficient. Your dad’s Playboy, your mom’s Cosmo and other magazines may have provided some insight, but were certainly not the gospel. Pornography offers a totally skewed perspective. As a consequence, most people have been educated through practical experience with their own vagina or with those of sexual partners. Although there is no substitute for “hands on” experience, a bit of vaginal academics is certainly a good addition to practical experience.
For many men—and women for that matter—the vagina is a dark and mysterious place, a “black hole” of human anatomy, hidden in the deep recesses of the body. This landscape is complex terrain and unfortunately does not come with a topographical map explaining its intricate subterranean geography.
The following are quotes about the vagina from Tom Hickman’s book: “God’s Doodle: The Life and Times of the Penis”:
“A place of procreative darkness, a sinister place from which blood periodically seeped as if from a wound.”
“Even when made safe, men feared the vagina, already attributed mysterious sexual power – did it not conjure up a man’s organ, absorb it, milk it, spit it out limp?”
The objective of this blog is to explore and demystify the vagina to help you comprehend and navigate its complexities. Knowledge is power and whether female or male, a greater understanding and appreciation of the anatomy, function and nuances of this curious and special female body part will most certainly prove useful.
Female Genital Anatomy 101
Table of Contents
The hidden female nether parts and their inner workings are a mystery zone to a surprising number of women. Many falsely believe that the “pee hole” and the “vagina hole” are one and the same…not surprising given that lady parts are much more unexposed, subtle and complex than the more obviously exposed man parts. However, what lies between the thighs is more complicated and intricate than one might think…. three openings, two sets of lips, swellings, glands, erectile tissue, muscles and more.
Let’s first set the record straight on the difference between the vagina and vulva, geography that is often confused. When referring to external visible “girly” anatomy, most people incorrectly speak of the “vagina”—this is actually the “vulva,” divided in half by a midline slit known in medical jargon as the pudendal cleft or cleft of Venus or in slang terms, “camel toe.” The “vagina,” on the other hand, is the internal, flexible, cylindrical, muscular passageway that extends from vulva to cervix (neck of the uterus). The vaginal opening on the vulva is known in medical terms as the vaginal introitus. Further down south is the landscape between the vulva and the anus known in medical jargon as the perineum or in slang terms, “taint.”
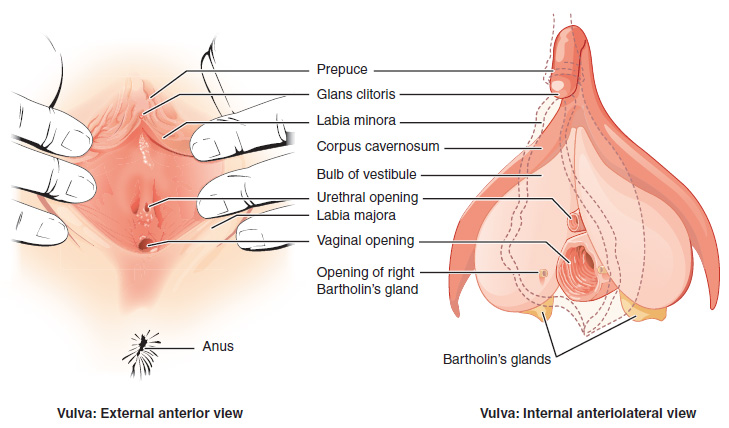
(Anatomy of the vulva by OpenStax College – Anatomy & Physiology, Connexions Web site., Jun 19, 2013., CC BY 3.0, no changes made to original)
Bottom Line: The vulva is external, the vagina internal. Good to remember.
Fact: The word “vulva” derives from the Latin “cunnus” (hence the derivation of the slang C-word. The word “vagina” derives from the Latin word for “sheath,” a cover for the blade of a knife or sword, an apt term.

Above image (public domain) entitled “Vagina Collage”…note that it should be entitled “Vulva Collage”
Many Functions Of The Vagina
The vagina is an amazingly versatile and multifunctional organ that is truly a “cave of wonders.” Beyond being a sexual organ, it is an inflow pathway and receptacle for semen, an exit pathway for menstrual blood, and a birth canal. It is not simply a passive channel, but an active and dynamic, highly responsive passageway that has the capacity for voluntary muscular contraction.
Anatomy Of The Vagina
The average depth of the vagina (without sexual stimulation) is 3-4 inches or so, but with sexual stimulation and arousal, the vagina is capable of considerable expansion and distension to a much greater potential. The elasticity of the vagina is truly impressive (perhaps the most elastic and stretchable organ in the body), with the ability to stretch to accommodate a full-term infant and then return to a relatively normal caliber. The width of the vagina varies throughout its length, narrowest at the vaginal opening and increasing in diameter throughout its depth. It is typically about 1 inch in diameter at the external opening.
Joke from Maxim.com:
- Just how deep is the average vagina?
- Deep enough for a man to lose his house, his car, his dog and half of all his savings and assets…
All vaginas are unique with a great variety in shape, size and even color, similar to variations in penile anatomy. The vagina is a banana-shaped structure and when a woman lies down on her back, the more external part of the vagina (closest to the vaginal opening) is straight, and the inner, deeper part angles/curves downwards towards the sacral bones (the lower part of the vertebral column that forms the back bony part of the pelvis). This vaginal “axis” often changes with aging and childbirth.
Banana representing vaginal axis, with inner portion curved towards sacrum and outer portion straight (Thank you Pixabay for image)
Fact: Although the vagina recovers remarkably well after childbirth, anatomy does generally change to some extent. Pelvic examination is usually easily able to distinguish between women who have and have not had children vaginally. Of note, elective C-section (no labor) preserves vaginal anatomy. Women who have an enlarged vaginal outlet due to childbirth may have difficulty in satisfactorily “accommodating” the penis, resulting in the vagina merely “surrounding” the penis rather than firmly “squeezing” it, with the end result being diminished sensation for both partners.
The vagina has pleats and corrugations called rugae that maximize the elasticity and stretchiness of the vagina. They are accordion-like ruffles and ridges that supply texture, which increase friction for the penis during sexual intercourse. In a young woman they are prominent, but with aging they tend to disappear.
Fact: Vaginal rugae are like tread on a tire…in young women they appear like deep grooves on a new snow tire, whereas in older women they appear like thinning tire tread, completely bald at their most extreme…aging can be cruel.
The vaginal wall has an inner lining of “skin” known as epithelium, which is surrounded by connective tissues and a muscular coat. The vaginal muscle is comprised of an inner layer that is circular in orientation and an outer layer that is oriented longitudinally. Contraction of the inner muscle tightens the vagina. Contraction of the outer muscle shortens and widens the vagina. The vagina is secured within a “bed” of powerful pelvic floor muscles.
To better understand vaginal anatomy, it is useful to divide it arbitrarily into thirds: outer, inner and middle. The outer and inner thirds are where “all the action is,” the outer third being the hub of sexuality, the inner third the hub of reproduction and the middle third essentially a connection between the inner and outer thirds.
Outer third: The outer third of the vagina is rich in nerve fibers and is the most sensitive part of the vagina. The “orgasmic platform” is the Masters and Johnson term for the anatomical “base” that responds to sexual arousal and stimulation with pelvic blood congestion. It consists of the outer third of the vagina and the engorged inner lips.
Middle third: The middle third is a conduit connecting the outer and inner thirds.
Inner third: The cervix (opening to the uterus) sits in the inner third of the vagina. Its presence within the deep vagina defines the deepest recesses of the vagina, which are referred to as the fornices (singular fornix), derived from the Latin word for “arches.” The largest fornix is the one behind the cervix (posterior fornix) with the two smaller fornices above and to the sides of the cervix (anterior and lateral fornices).
Question: What do you think is the origin of the word “fornicate”?
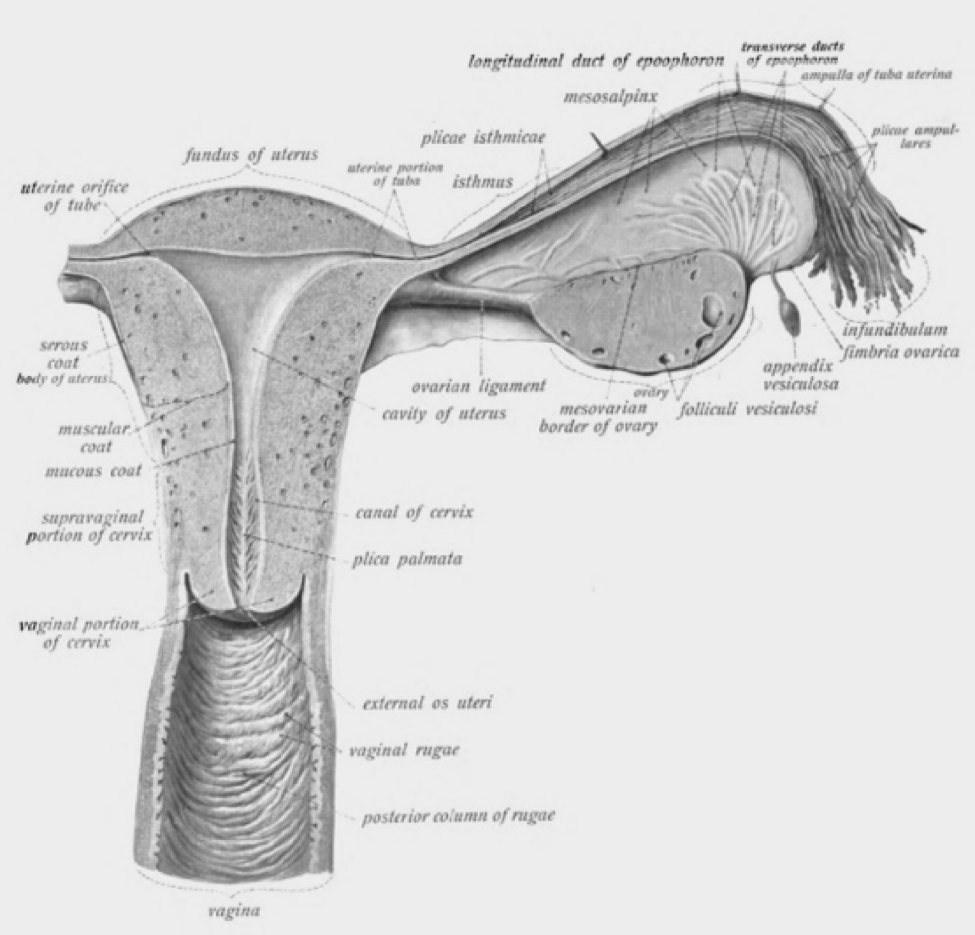
Image above: Uterus, Cervix and Inner Third Vagina from Dr. Johannes Sobotta – Sobotta’s Atlas and Text-book of Human Anatomy 1906, note the vaginal rugae and the relationship of the cervix with the inner vagina
Fact: In the man-on top sexual intercourse position, the penis reaches the anterior fornix, while in the rear-entry position it reaches the posterior fornix.
The Pelvic Floor Muscles And The Vagina
The pelvic floor muscles play a pivotal role with respect to vaginal and sexual function, their contractions facilitating and enhancing sexual response. They contribute to arousal, sensation during intercourse and the ability to clench the vagina and firmly “grip” the penis. The strength and durability of their contractions are directly related to orgasmic potential since the pelvic muscles are the “motor” that drives sexual climax and can be thought of as the powerhouse of the vagina. During orgasm, the pelvic floor muscles “shudder.”
There is great variety in the bulk, strength, power and voluntary control of the pelvic floor muscles that support the vagina. Some women are capable of powerfully “snapping” their vaginas, whereas others cannot generate even a weak flicker.
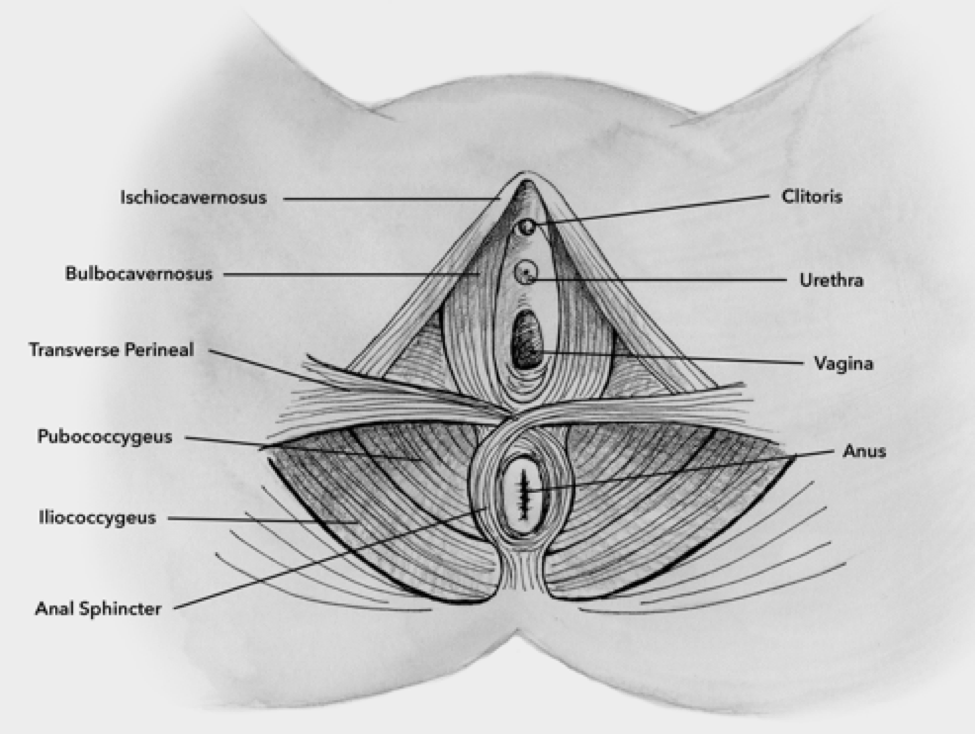
Image above: Female pelvic floor muscles, illustration by Ashley Halsey from The Kegel Fix
Fact: “Pompoir” is a sexual technique in which a woman contracts her pelvic floor and vaginal muscles rhythmically to stimulate the penis without the need for pelvic motion or thrusting. Women who diligently practice Kegel exercises can develop powerful pelvic floor muscles and become particularly adept at this technique resulting in extreme vaginal “dexterity” and the ability to refine pulling, pushing, locking, gripping, pulsing, squeezing and twisting motions, which can provide enough stimulation to bring a male to climax.
Fact: “Penis Captivus” is a rare condition in which a male’s erect penis becomes stuck within a female’s vagina. It is thought to be on the basis of intense contractions of the pelvic floor muscles, causing the vaginal walls to clamp down and entrap the penis. It usually is a brief event and after female orgasm and/or male ejaculation, withdrawal becomes possible. However, it sometimes requires medical attention with a couple showing up in the emergency room tightly connected, like Siamese twins. Not a good call to 911!
Sexual Function And The Vagina
Under normal circumstances, the vagina is not “primed” for sex and is little more prepared for intercourse than is a flaccid penis. The un-stimulated vagina is essentially a closed “potential space” in which the vaginal roof and floor are in contact. With sexual stimulation, the vagina expands with lengthening and widening of its inner two-thirds and flattening of the rugae. The cervix and uterus pull up and back. Pelvic blood flow increases and the vaginal walls undergo a “sweating-like” reaction as a result of pelvic blood congestion, creating a slippery and glistening film. Most of the lubrication is based upon seepage from this increased blood flow, but some comes from Bartholin’s and Skene’s glands. Bartholin’s glands are paired, pea-size glands that drain just below and to each side of the vagina. During sexual arousal they secrete small drops of fluid, resulting in moistening of the opening of the vagina. Skene’s glands are paired glands that drain just above and to each side of the urethral opening. They are the female equivalent of the male prostate gland and secrete fluid with arousal.
With sexual excitement and stimulation, in addition to vaginal lubrication from increased pelvic blood flow, there is congestion and engorgement of the vulva, vagina and clitoris.
Fact: The profound vaginal changes that occur during sexual arousal and stimulation are entirely analogous to the changes that occur during male arousal: expansion of penis length and girth, retraction of the testicles towards the groin, and the release of pre-ejaculate fluid.
With increasing stimulation and arousal, physical tension within the genitals gradually builds and once sufficient intensity and duration of sexual stimulation surpass a threshold, involuntary rhythmic muscular contractions occur of the vagina, uterus, anus and pelvic floor muscles, followed by the release of accumulated erotic tension (a.k.a. orgasm) and a euphoric state. Thereafter, the genital engorgement and congestion subside, muscle relaxation occurs and a peaceful state of physical and emotional bliss and afterglow become apparent.
Fact: Anatomy can affect potential for experiencing sexual climax.
Sexual intercourse results in indirect clitoral stimulation. The clitoral shaft moves rhythmically with penile thrusting by virtue of penile traction on the inner lips, which join together to form the hood of the clitoris. However, if the vaginal opening is too wide to permit the penis to put enough traction on the inner lips, there will be limited clitoral stimulation and less satisfaction in the bedroom. Furthermore, studies have suggested that a larger clitoris that is closer to the vaginal opening is more likely to be stimulated during penetrative sexual intercourse.
At the time of sexual climax, some women are capable of “ejaculating” fluid. The nature of this fluid has been controversial, thought by some to be hyper-lubrication and others to be Bartholin’s and/or Skene’s gland secretions. There are certain women who “ejaculate” very large volumes of fluid at climax and studies have shown this to be urine released because of an involuntary bladder contraction that can accompany orgasm.
Fact: “Persistent genital arousal disorder” is a rare sexual problem characterized by unwanted, unremitting and intrusive arousal, genital engorgement and multiple orgasms without sexual interest or stimulation. It causes great distress to those suffering with it and there are no known effective treatments. It typically does not resolve after orgasm.
The G-Spot—named after German gynecologist Ernst Grafenberg—was first described in 1950 and was believed to be an erogenous zone located on the upper wall of the vagina, anatomically situated between the vagina and the urethra (urinary channel). Stimulation of this spot was thought to promote arousal and vaginal orgasm.
Fact: There is little scientific support for the existence of the G-spot as a discrete anatomical entity; however, many women feel that they possess an area on the roof of the vagina that is a particularly sensitive pleasure zone. Although its existence remains controversial, the G-spot is certainly a powerful social phenomenon.
Regular sexual activity is vital for maintaining the ability to have ongoing satisfactory sexual intercourse with the vagina staying fit and healthy if one remains sexually active, as nature intended. Vaginal penetration increases pelvic and vaginal blood flow, optimizing lubrication and elasticity, while orgasms tone and strengthen the pelvic floor muscles that support vaginal function. “Disuse atrophy” is a condition when the vagina adapts to not being used, with thinning and fragility of the vaginal walls and weakness of the pelvic floor muscles. Use it or lose it!











{kind=link}